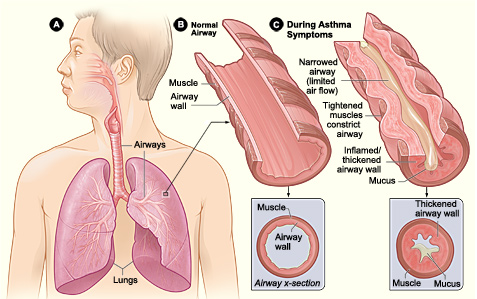
 Asthma is an inflammatory disease of the airways; affecting 5.9 million people in the UK (Asthma UK 2011). There are two asthmatic forms: Intrinsic and Extrinsic. Extrinsic asthma affects children and over 80% of its deaths occur in developing countries. However, it can occur anywhere regardless of development levels (WHO, 2011). Intrinsic asthma affects elderly. Amongst the common symptoms of asthma are wheezing, coughing and dyspnoea (breathlessness). Dry coughing associated with wheezing due to bronchoconstriction and causes sleep disturbances particularly in the early hours (Munro, 2000:118). These clinical features are the outcome of a complex cascade of events in the inflammatory mechanism proceeding, including structural and biological changes after her airways were exposed to a stimulus. For instance, dust. Normally, inhaled antigens are eliminated by mucociliary escalator mechanisms in the tracheobronchial tree. The escalator consists of mucous-producing goblet cells and ciliated epithelium. It removes particles that sediment the airways by cilia continuously beat and transfers adhesive mucus containing antigens out and up the larynx to the epiglottis to be swallowed (University of Colorado, 2011). Asthma is diagnosed via taking a medical history and breathing tests to ensure how well lungs are working. A spirometry is a test where you take a deep breath and blow into a sensor. This test measures the amount of air the lungs is needed to hold and the speed of the air for inhaling (breathing in) and exhaling (breathing out. It ensure examines how severe the asthma is and whether the treatment is working. An allergy test may also take place to see what triggers your asthma. This could be animal fur, dust, pollen, nut or something that will trigger your asthma. Thus, identifying what triggers your asthma will aid in helping to manage your asthma. Is there are treatment for asthma? Symptoms experienced can be controlled using effective treatment and management.Amongst are the following: leukotriene modifiers: These are oral medications that help relief quickly symptoms and helps relax and open the airways. Controller medications: These are taken daily. Examples include inhaled corticosteroids such as beclomethasone, fluticason, mometasone. Combination inhalers: This consists of inhaled corticosteroids and a long-acting beta-agonist. LABAs controls the symptoms and opens the airways. However, it has side-effects and thus it is never prescribed solely for asthma and thus is used alongside corticosteroids. Examples of combination inhalers are (salmaterol and fluticasone). Oral and intravenous corticosteroids – This is needed for severe symptoms. Examples include prednisone. 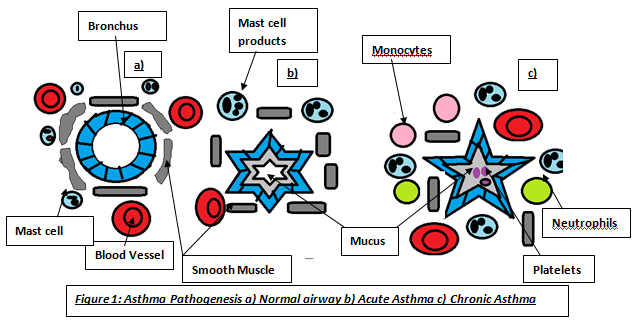 WANT TO DIP DEEP INTO ASTHMA?The pathophysiology of asthma is divided into early and late phase reactions. The early phase causes a forced expiratory volume in 1 second, whereas, in the late phase causes a decrease in bronchial airflow for 4-8 hours (Fireman, P. n.d.). The inflammatory cells responsible for most clinical symptoms are mast cells, basophils, eosinophils and lymphocytes. The inhaled allergens penetrate the respiratory epithelium and are captured by dendritic cells. The antigens are presented to the B and T lymphocytes. The B-lymphocytes produce Immunoglobulin E (IgE) which is dependent on CD4 T-cells (Price 2004:14). This is immediate hypersensitivity. IgE is a monomer consisting of two heavy chain containing four C-domains, and two light chains (Wood 2001:47). The cells differentiate into Th2 cells secreting interleukin-4 (IL-4) responsible for allergen-specific IgE production. The Fc part of these allergens bind to the F¢εR receptors on membrane surfaces of mast cells (Wimberly 2001:148). Mast cells are responsible for the initial inflammatory response due to their residence in tissues; however, there are two types with different properties: mucosal found in the lungs, whereas, connective found in most tissues (Wood 2001:233). This binding activates and degranulates mast cells releasing mediators into the blood. There are two types of anaphylactic mediators: Preformed stored in granules of mast cells and basophils; histamine and enzymes. Newly-generated mediators produced after mast cell activation; arachidnoic acid metabolites. Phospholipase releases arachidonic acid from phospholipids and are exposed to enzymes making metabolites: LTC4 and PGD2. These mediators cause Ruby’s allergic manifestations and can cause acute asthma attacks.
The late phase is due to influx of other inflammatory cells that further stimulate mucus secretion, epithelial cell damage and activation of platelets leading to microthrombi in the airway (Wood 235), characterized by airway inflammation leading to epithelial denudation, cellular infiltration, submucosal oedema and increased collagen deposition under the epithelial basement membrane. An increase in collagen also produces sub-basement fibrotic effects which remodels airway with irreversible obstructions (Clark 1998:9). Microscopically, asthma is characterized by the presence of increased numbers of eosinophils, neutrophils, lymphocytes, and plasma cells in the bronchial tissues, bronchial secretions, and mucus. Four events during inflammatory response|: vasodilation cause increase blood flow, increase supply of cells...activation of endothelial cells making them more sticky to blood cells, increase vascular permeability-cells and proteins pass through vessel wall. Mast cells also release enzymes that degrade blood vessel endothelial membrane. Tryptase, a serine protease has high abundance and are used in studies regarding asthmatic response evaluation. Its large structure allows slow movement around the inflammation site and enhances histaminic effects by: basement membrane thickening. It also degrades both bronchoactive peptides and vasoactive intestinal peptide that inhibits smooth muscle relaxation and causes over-proliferation of epithelium respectively. It can act as an anticoagulant transporting inflammatory cells to the injury site. These roles cause significant structural changes of the airway and bronchoconstriction. Wheezing are sounds produced by air passage through narrowed bronchi (Munro 123) wheezing is louder during expiration and often confided . it is more conspicuous and audible only during deep breathing.. patients with stridor can also get wheeze. Care needs to be distinguished between two sounds as stridor is caused by partial obstruction of a major airway (e.g laryngeal oedema, tumour and needs urgent treatment (Munro 123) Another enzyme is chymase which is not abundant as tryptase but have similar roles. For instance, neuroactive peptides degradation and vascular permeability increasing inflammation as serum proteins and fluid travel across endothelium. Matrix proteins degradation causes epithelial damage (Wimberly 2001:149). Basophils can bind to IgE. Basophils and IL-3 originates in the bone marrow stimulating cell differentiation and binds to IgG. Its granules contain histamine and IL-4. Histamine is produced via histidine decarboxylase. Its effects on lung tissue depend on receptor stimulated. The H1 receptor on smooth muscle causes muscle contraction leading to bronchoconstriction and airway oedema (Wimberly 2001:149). This caused Ruby’s prolonged breathless at hospital. Increases work of breathing, increase ventilator drive and imapaired respiratory muscle function (Jamison 120) This condition is called bronchospasm. Eosinophils invade the bronchial wall resulting in airway becoming oedematous (Clark 1998:9). The H2 receptors causes yellow, viscid and regulates histamine release via negative feedback. Mucus hypersecretion can lead to plugging due to mucus and desquamated epithelial cells and the sputum can be coughed up in acute attacks (Clark 1998:9). Other manifestations include watery eyes and nasal discharge. Another histaminic role is antibody and prostaglandin hypersecretion. Prostaglandin (PGD2) is a bronchoconstrictor and can also be synthesized by cyclooxygenase pathway (COX) to make prostaglandins and thrombaxane b2 Another bronchoconstrictor is LTC4 a leukotriene produced by 5-hydroperoxyeicosatetraenoic acid in lipoxygenase. LTC4 becomes a contractile agonist at the CisLTs receptor, located on the bronchial smooth muscle resulting in bronchoconstriction. (Wimberly 2001:149). Tumour necrosis factor-α, IL-4, IL-5, IL-6 are cytokines are important in asthmatic attack propagation. TNF-α is secreted in mast cells and increases adhesion molecule levels (selectins – bind to sugars on mucins, integrins-bind to ICAMScausing leukocytes activation and adhesion of: eosinophils, basophils and neutrophils to endothelium and migrate to the injury site promoting inflammation. Besides IgE synthesis, IL-6 is involved in reducing cytokine effects. IL-5 involves eosinophil production abundant in alveolar lavage fluid. For eosinophil and macrophage maturation, T –cells release IL-3, IL-5 and granulocyte-macrophage colony-stimulating factor (GM-CSF). These cells are critical for prolonged asthmatic response due to acculumation of these leads to epithelial denudation and airway oedema they are inactivated form and lose granules after allergen clark p102. Denudation is caused by major basic protein (MBP) located in eosinophil granules, whereas, oedema results from epithelial damage from MBP. Epithelium produce epithelin which is a bronchoconstrictor and vasoconstrictor, nitric oxide is a vasodilator and bronchodilator. NO production may be stimulated by cytokines and NO produced has cytoxic effects on epithelium (clark 102). Bronchoconstriction may be caused by MBP enhancing effect of cholinergic contraction of airways. Cholinergic effects on lungs via acetylcholine cause bronchoconstriction, mucus hypersecretion and bronchial vasodilation. If airways are not hyper-responsive, cholinergic effects maintains airway tone through vagus nerve and increases vagal output which normally occurs during stress or at night. This emphasises why she was breathless when she was distressed. Chonlinergic fibres constrict smooth muscle, stimulation of beta adrenoreceptors dilates muscle, little adrenergic nerve supply bronchials smooth muscle so adrenaline provides main stimulus to thesr receptors. Third system is nonadrenergic, noncholingeric system that has transmitters that produce constriction or dilation, inflammatory mediators may affect release of neutrotransmittors (clark 103)Besides these cells, studies have shown that chemotactic factors such as eotaxin have shown to be eosinphil chemoattractants and eosinophils promote pathophysiological dysfunction including peribronchial thickening and fibrosis (Nature, 2011) Studies show that lymphocytes are important in orchestration of inflammatory response rather than sources of mediators (Clark 102). Macrophage originates from blood monocytes and must be present for T-cell activation and secrete cytokines and chemotactic factors all involved in asthmatic airway response clark 102. This occurs through a signal passed between the B7 molecule located on macrophage and the CD28 molecule on the T cell. For instance, IL-1, IL-6 and TNF-β. IL-1 enhances T and B-cell activation and increase capillary permeability allowing inflammatory components to migrate neutrophil/polymorphonulear leukocyte to injury site increasing oxidant levels. Oxidants potentiate the airway causing epithelial damage, bronchoconstriction, and decreased ciliary action leading to airflow obstruction. IL-1 causes an increased production of other cytokines. TNF-β stimulates cytokine production and increase endothelial permeability to facilitate blood cells movement to injured site.
0 Comments
Leave a Reply. |
This project began as a facebook page sharing information about different illnesses, diagnosis and treatments. We are now doing short articles :)
Health stuffArchives
April 2020
Categories |
 RSS Feed
RSS Feed
