|
A high-tech comparison of the breast milk of humans and their close primate relatives is revealing just how nutritious the human variety is.
The research was led by Danielle Lemay, a nutritional biologist at the University of California, Davis' Genome Center. Her team used a new technique for identifying proteins found in breast milk. The researchers found that human breast milk has far more protein content than the breast milk of one of humans' closest primate relatives, the rhesus macaque monkey. "The higher levels of these proteins in human milk are consistent with the well-established perspective that human babies, compared to other primate infants, are born at a slightly earlier stage of development and require higher levels of specific proteins that will nurture them as they mature," Lemay said in a university news release. In other words, human breast milk might be even more protein-rich because human babies rely on its nutritional benefits to a larger degree than other primates. Lemay and her colleagues published the findings online this month in the Journal of Proteome Research. The new research relies on a new means of molecular analysis that enabled the team to spot more than 1,600 distinct proteins in human milk, of which more than 500 were spotted for the first time. This compared with just over 500 proteins found in rhesus macaque milk. The breast milk of humans and rhesus monkeys also share 88 proteins in common, the team noted. However, 93 percent of those shared proteins were still found in higher quantities in human milk. Some of those proteins aid in the digestion of fats, Lemay's team said, while others boost babies' ability to absorb iron and vitamins B-12 and D. Current recommendations from the American Academy of Pediatrics urge women to breast-feed their baby exclusively for the first six months of life, and then combine breast milk and other foods until at least 12 months. Going forward, Lemay suggested that "proteins that appear to have neurodevelopmental significance for human babies will be key targets for future research focused on enhancing infant formula." Source:http://www.medicinenet.com/script/main/art.asp?articlekey=187731
0 Comments
“A mans true wealth is the good he has done in this world” Prophet Muhammad (Peace be with him) If there is one thing that all human beings have in common, it is that we contain rich red blood nourishing us all with life. A bountiful source for some and desperate need for others. With the necessity for the fortunate people in our world to gear their efforts in dedicating their energies to helping those of us in strife, voluntary blood donation nurtures unity amongst a community, a nation and the human race and it only starts with one drop. Blood banks highlight that the importance of blood donations for hospitals and health care service providers is to have continuous availability of varied blood types that are safe suitable and effective for patient use. This minimises the chances of delay of blood transfusions day to day especially during emergencies. According to the NHS U.K, doctors, surgeons and health care practitioners depend on blood donations to perform life-saving procedures and life-enhancing treatments every day. Around the world, HIV/AIDS, malaria and maternal mortality rates decrease due the availability of blood donations. The most incredible thing is that every average healthy person weighing (above 50kg) between the age of 17 and 66 has around 5 trillion red blood cells in one litre of blood. Therefore approximately 25 trillion red cells in the average amount of blood in an adult which accounts to 5 litres! The NHS confirms that about 450mls of your 5 litre store is taken for donation. Not much at all for your healthy body but a lot for 3 people suffering. In addition to the remarkable ways of our blood stores, is that our body makes about two million new red blood cells every second, which goes to show our stores are replenished very quickly after donating. Top uses of Blood donations Cancer and blood diseases- 34% Surgical- 30% Haematology- 18% Gastro intestinal bleeding- 11% Anaemia- 30% Maternity- 6% Other- 5% The main uses of blood are; · Red blood cell transfusions are used to make up for heavy blood loss usually as a result of accidents, surgery and childbirth. In other cases it is effective in treating severe anaemia. · White blood cells work to fight infection. Transfusions of this kind in cases of leukaemia- The cancer of the bone marrow which is due to the replication of abnormal white blood cells which over time takes the place of the normal functioning cells, known as leukaemia cells, impairing the role of blood cells in fighting life threatening infections. · Platelets assist our blood to clot after injuries. If they are not functioning normally or are low then the patient may suffer a lot from bruising and bleeding. · Plasma consists of two essential components i.e. Albumin which plays a role in transport of essential molecules in the blood. Incase a large amount of blood is lost by a patient it must be made up for to maintain normal functioning of the body. And clotting factors which are important in clotting of blood. · Immunoglobulins are a type of antibody that protects you from future infection and disease. For example a child who has suffered from chicken pox will have a supply of chicken pox antibodies therefore their plasma will be ideal for children with leukaemia who have been exposed to chicken pox, and also to prevent any potentially life-threatening diseases. Who can donate? · Be at least 16 or 17 years of age · Weigh at least 110 pounds · Be in good health Who cannot donate? · Low blood cell count · During pregnancy and until 6 weeks after giving birth · Having received a tattoo or any body piercing within the past year Brief donation procedures: Before the donation it is recommended to; · Eat regular meals rich in Iron · Rest well · Drink plenty of liquids and abstain from alcohol During the blood donation you will receive check up on your; · Pulse · Blood pressure · Body temperature · Haemoglobin Note: Who can donate or cannot as well as the donation procedures depends on your doner servie provider. The above information is just a guidance of what to expect. QUICK BLOOD FACTS 1. Highest use of blood donations is for cancer and blood diseases- 34% 2. B-, AB+ and AB- are the rarest blood types 3. 25 trillion red cells in the average adult boy which equals 5 litres! 4. 450mls of your blood will help 3 people 5. Blood cannot be manufactured but it can be given for free In conclusion, the opportunity to donate one’s blood is a step into a transforming lifesaving venture which is worthy of emulation today and generations to come. YOUR blood can be the reason someone you know or do not know; breaths longer, hugs tighter and smiles wider. With a constant need to get blood there is an instant happiness in giving it <3 Give blood. Give life! Save a life. Give blood!  Energy drinks might give you some pep — but they might also be priming you for heart problems, a new study finds.
Researchers found that energy drinks can raise blood pressure to potentially unhealthy levels. The effect was far more prominent in young adults who did not consume caffeine regularly, according to the study, presented March 14 at an American College of Cardiology meeting in San Diego. In this study, the research team — led by Dr. Anna Svatikova, a cardiovascular-diseases fellow at the Mayo Clinic in Rochester, Minnesota — gave a can of a commercially available energy drink to 25 healthy volunteers, whose ages ranged from 19 to 40. On a different day, the participants drank the same amount of a placebo drink. The researchers measured the participants' heart rate and blood pressure before and after the drinks. The participants experienced a more marked rise in blood pressure after consuming the energy drink than after drinking the placebo, according to the findings. The participants' average systolic blood pressure (the top number in a blood pressure reading) increased by 3 percent more after they drank an energy drink, compared with after they drank the placebo drink. The effect was most dramatic in people who did not typically consume more than a small cup of coffee or other caffeinated drink daily. In this so-called "caffeine-naive" group, the blood pressure increase was twice as high as the increase seen in the people who drank at least the equivalent of a cup of coffee on a daily basis, the researchers said in a statement. Even a small increase in blood pressure can have deadly consequences, depending on your age and resting blood pressure, said Sachin Shah, an associate professor of pharmacy at the University of the Pacific in Stockton, California, who was not involved in the study. "An acute, moderate increase in blood pressure is typically not a cause of worry in healthy subjects," said Shah, who has done research on the effects of energy drinks. However, in older people or those with hypertension, a moderate increase may be a cause for concern, he said. At a population level, an increase of three or four points on a systolic blood pressure reading could mean a significant increase in deaths from stroke. Scientists do not know whether it is the caffeine, taurine or other ingredients found in energy drinks — or a combination of ingredients — that can adversely affect the heart. In a separate study, presented last year at an American Heart Association meeting by Maj. Emily Fletcher of the David Grant Air Force Medical Center, healthy volunteers experienced a greater increase in blood pressure after they consumed an energy drink compared to after they drank a coffee drink that had an equal amount of caffeine. This result, Fletcher said, suggests that ingredients in the energy drink other than caffeine were conspiring to raise blood pressure. According to the Mayo Clinic, consuming up to 400 milligrams of caffeine a day appears to be safe for most healthy adults. That's roughly the amount of caffeine in four cups of brewed coffee, 10 cans of cola or two "energy shot" drinks. Previous studies have associated the consumption of energy drinks with poor memory and learning, anxiety, hallucinations, abnormal heart rhythm, substance abuse, and risk-taking behaviors. A study published in the journal Pediatrics in 2011 found that children, in particular, are at high risk of cardiac abnormalities from consuming energy drinks because of their smaller body size. Atherosclerosis is the development of atheromatous plaques in the inner arterial wall. It is the underlying reason for the pathophysiology and aetiology of many arterial diseases particularly coronary artery disease (CAD) where these plaques partially or completely block arteries. This limits the oxygenated blood supply to myocardium causing over 90,000 UK deaths a year despite rates decreasing since 1970s (BHF,2009). There are two main coronary arteries (right and left) arising from aortic sinus; the anatomy of coronary artery is shown in Figure 1a. 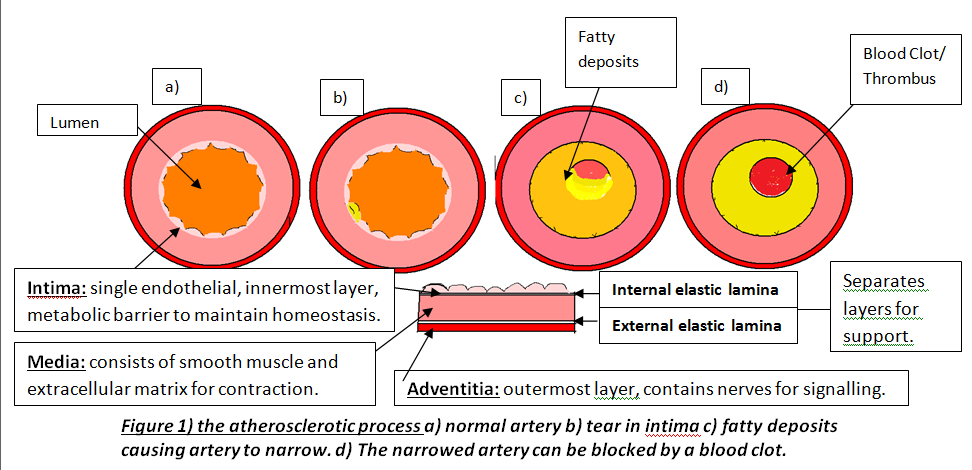
Atherosclerosis occurs in three major stages: fatty streak, plaque progression and disruption. Factors such as smoking cause endothelium to produce superoxide anions that interacts with other molecules. Superoxides are reactive oxygen species and free radicals of dioxygen due to unpaired electron (Widmaier,E. 2008:pp.84). This causes oxidative stress leading to endothelium dysfunction, allowing lipoproteins, calcium and fibrous tissues to enter and modify intima; Figure 1b. This initial damage increases CAD risk and initiates leukocyte recruitment primarily monocytes and T lymphocytes to enter inflammatory site. Monocytes differentiate into macrophages and secrete growth factors, platelet-derived growth factor (PDGF) and transforming growth factor-β (TGF- β), and have LDL-receptors to engulf lipids forming foam cells (Lilly,L. 2007 pp.126). These foam cells accumulate to form yellowish fatty streaks; Figure 1c. Plaque growth progresses when smooth muscle migrates to intima. PDGF allows smooth muscle to proliferate for collagen synthesis whereas TGF- β stimulate the process losing the arterial wall’s elasticity (Lilly,L. 2007:pp.127). A fibrous cap forms protecting atheroma, causing an ischaemic condition called angina. Over decades, dispute occurs between growth factors and IFN-γ factor; an interferon released by leukocytes inhibiting collagen synthesis. Disruption occurs when plaques rupture triggering a coagulation cascade where thrombus and fibrin deposit in arterial wall further reducing lumen and cause coronary occlusion; Figure 1d. This can lead to myocardial infarction (MI) where inadequate blood supply to part of the heart causes myocardial necrosis and can be fatal. Other causes of CAD are risk factors that promote atherogenesis. Controllable factors include diet, exercise and obesity. Obesity increases risk because abdominal fat enhances low-density lipoproteins (LDL) production and heart workload. Studies show that a third of CAD patients in developed countries are due to obesity emphasising its impact (BHF, 2008). As well as being an independent factor, it can trigger other factors, for instance, cholesterol where high LDL and triglyceride levels inside coronary arteries increase plaque formation. Low high-density lipoproteins (HDL) levels raises risk because epidemiological studies show that high HDL levels enhances endothelium function by preventing cholesterol entry (Brubaker,P. 2002:pp.9). There are also uncontrollable factors that contribute to CAD, for instance, gender and age. Women have higher HDL2 levels, a more cholesterol rich, than men preventing cholesterol entry and lowering CAD risk. Studies show 40% of deaths in 65-74 years old are due to CAD because myocardium cardiac function has decelerated, myocardium becomes less efficient and cardiac muscle (BJN, 2009). Individuals at risk of CAD are diagnosed using different examinations after experiencing symptoms such as chest discomfort where it spreads to arms and other areas; MI is identified when discomfort is beyond 15 minutes (Julian,D. 2005:pp.116). Clinical history and electrocardiogram (ECG) is needed because ECG records heart’s electrical activity by placing electrodes on arms, legs and chests detecting characteristic changes. For instance, ST segment lowers when there is myocardial ischaemia but elevates when MI initiates; Figure 2. 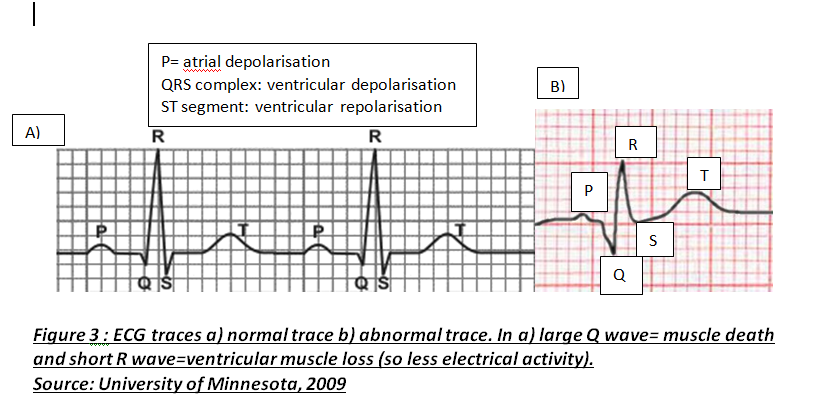
Another diagnosis is cardiac markers where high enzyme concentrations in cardiac tissues indicate myocardium necrosis. Tropinin T and I regulate cardiac muscle contraction and are mainly tested because they are sensitive and raise their serum activity when they detect any muscle injury (Julian,D. 2005:pp.112).
Treatment of CAD aims to improve coronary circulation by dilating coronary arteries which lowers pressure and myocardial oxygen demand and this reduces heart work. Drugs like nitrates have this pharmacological effect by relaxing smooth muscle whereas other drugs like atorvastatin lower LDL cholesterol by inhibiting HMG-CoA reductase; enzyme responsible for cholesterol synthesis (Kendall,M. 1998:pp.109). However, atorvastatin can cause myositis which affects muscles emphasising how medications can cause side-effects. If medications fail to work, surgery is needed. Coronary artery bypass grafting (CABG) involves using a vessel, normally saphenous vein, which bypass narrowed arteries providing an alternative route for blood flow. In 2002, mortality rate for Coronary Artery Bypass operations was 1.8% highlighting how surgery is effective (Barrett,D. 2006:pp.212). However, studies show that preventing modifiable factors by lifestyle adjustments are more effective than other treatments. Stopping smoking, maintaining healthy weight by exercising and eating low-saturated fat diet helps reduce cholesterol, blood pressure and controls glucose levels if diabetic. Ultimately, researchers are investigating possible new factors and cardioprotective drugs which emphasises the epidemic’s extent. Advanced understanding in the molecular aspect of disease generated progress leading to a novel healthcare approach called stratified medicine. From recent years it transitioned from several stratified medicines such as Imanitib, a mutant kinase inhibitor prescribed for patients with chronic myeloid leukaemia to a variety of medicines today such as Zelboraf; targets BRAF proteins in patients with V600E mutation in melanoma. Stratified medicine is defined as a treatment derived from utilizing molecular or genetic information to discover patients with different mechanisms of disease or a specific therapeutic response as illustrated in Figure 1. This allows identification and development of therapies and diagnostic tools that give better health stances such as safety and effectiveness, for an aimed sub-group of patients that have analogous biological characteristics. Besides patients, there are also benefits for clinicians, economics and healthcare system. Thus, stratification plays a significant role in medicine especially cancer therapy. 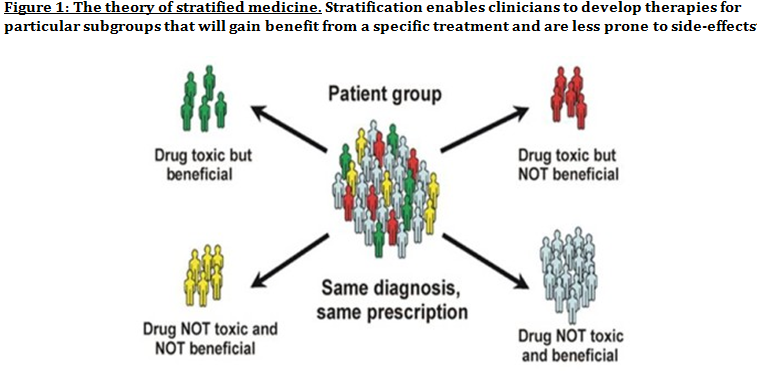 One of the ways in which stratified medicine alters cancer treatment can be seen through HER-2 status in breast cancer management illustrated in Figure 2. This is where findings from prognosis research are translated towards developing better patient outcomes. At first, HER-2 protein was found as a prognostic factor due to overexpression in breast cancer cells. This led to development of Trastuzumab (Herceptin) as a potential treatment against HER-2. Then, evaluation in trials took place where subjects recruited were women with HER-2 positive cancers. Due to successful results, Herceptin was prescribed to HER-2 positive patients and not those that were HER-2 negative. Those that were negative had alternative treatments. 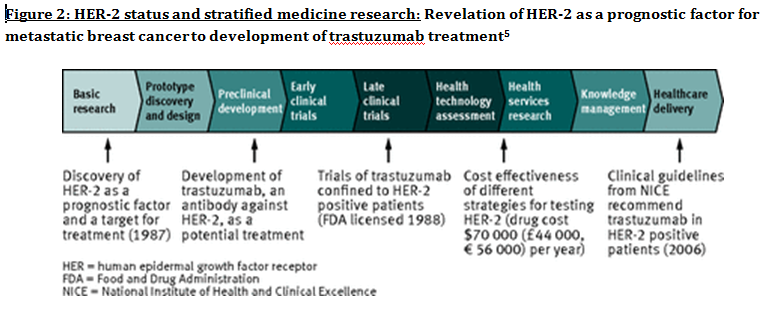 Another way in which stratified medicine is altering cancer treatment is via biomarkers. Biomarkers are defined as biological characteristics that give an indication of pathogenic process, normal biological state or pharmacological response to a therapeutic involvement. They can be cellular, biochemical or genetics. These markers allow identification of sub-groups that are able to respond positively or negatively due to a particular treatment. A number of randomised control designs (RCT) are used to assess predictive biomarkers such as biomarker-strategy design presented in Figure 3A. They are utilized in scenarios where there are two or more therapeutic options8. Patients are assigned on a random basis despite of their biomarker status8. An analysis plan is then stratified via biomarker to examine the treatment effect. An example of this is Marker Validation for Erlotinib in Lung Cancer (MARVEL) trial8. Patients with non-small cell lung cancer (NSCLC) are allocated to either treatment: Pemetrexed or Erlotinib. The analysis plan is then stratified via epidermal growth factor receptor gene (EGFR) status. This is followed by qualitative analysis via fluorescent in situ hybridization (FISH). Advantages of using biomarker-strategy design are that it examines relative efficacy of each sub-group. However, it is unreasonable for multifaceted therapeutic approaches and several treatments maybe inappropriate for some biomarker groups. Another type of RCT design is Enrichment design (Figure 3B), it consists of evaluating all patients, however the analysis plan is stratified to specific patients with definite biomarker values8. For example in CALGB-10603 trial, utilized a predictive biomarker allowing only acute myeloid leukaemia patients with FLT3 mutation. They were allocated randomly to a normal treatment or a treatment that entailed FLT3 kinase inhibitor; midostaurin, whereas, those without FLT3 mutation where ‘off-study’. One of the benefits of using enrichment design is that it utilizes a small sample. Nevertheless, it requires potent biological basis and the biomarker may not identify correctly the sub-group that would gain. Additionally, biomarker-strategy design (Figure 3C) entails patients who are allocated randomly and uses an investigational treatment arm that utilizes biomarker to direct treatment or to a control arm that does not direct treatment8. An example of this can be seen with Excision repair cross-complementing 1 (ERCC1) as biomarker. It is linked to cisplatin resistance in NSCLC. Therefore, in the trial patients are allocated on a random basis to the control arm8. This is where they will be given two treatments: docetaxel and cisplatin8. However patients may be allocated to the biomarker-strategy arm where patients are altered to gemcitabine and docetaxel treatment rather than being categorized as cisplatin resistant. Patients thare are not resistant to cisplatin undergo the standard treatment which is composed of cisplatin and docetaxel. This design can be used in complex therapeutic approaches. On the contrary, a positive trial does not demonstrate biomarker use. This emphasises the clinical relevance of biomarkers towards cancer treatment. However, there are disadvantages of utilizing biomarkers such as insufficient handling, processing and storage of samples. This can lead to their degradation and false results. For improvement, removal of quality samples for biomarker analysis from reliable sources reduces issues to patients. This will need design and validation of protocols for procedures. 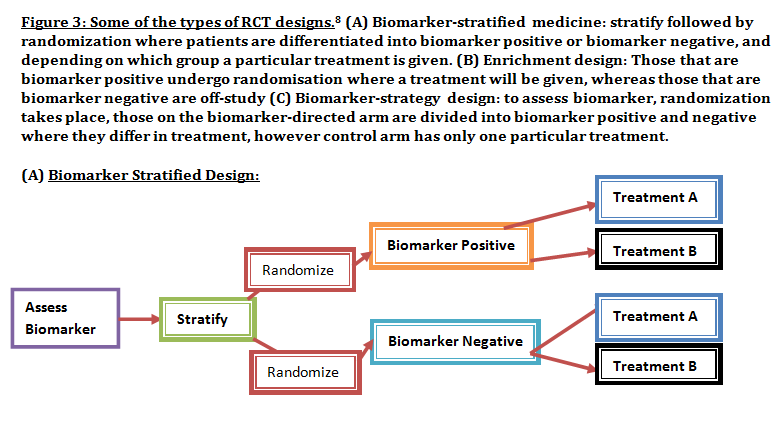 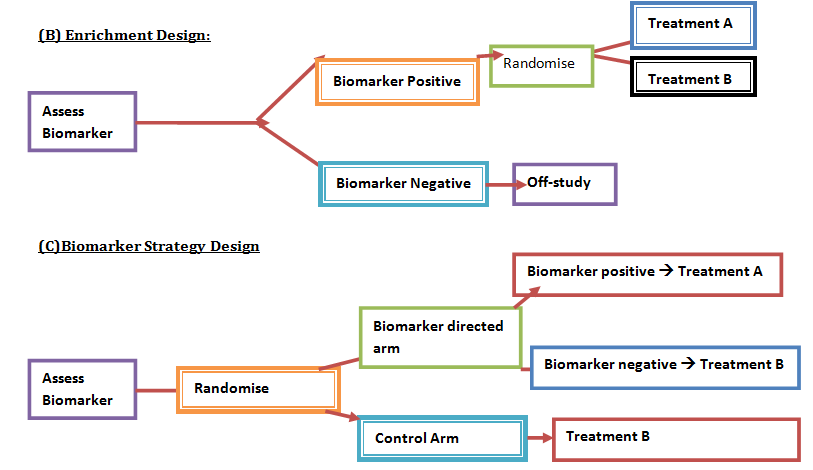 A technique in which cancers can be stratified is genomic analysis using DNA and RNA microarrays. Microarrays consist of RNA or DNA pieces from genes and quantify the amount of corresponding DNA or RNA in the provided sample. Therefore, genetic variants or expression levels of disease-related genes can be observed. For example MammaPrint, a microarray-based diagnostic technique can examine genetic variants in breast cancer tissue to estimate possibility of metastasis. However, microarrays are limited because they can only assess genes presented there. DNA microarrays will potentially be substituted with whole genome sequencing due to benefit of obtaining complete information, whereas RNA microarrays remains valuable for exploring gene expression. Moreover, metabolomic and protein analyses are another method used to stratify patients. Microarrays can be utilized where antibodies fuse to desired metabolite or protein variant. In comparison to genomics, both analyses provide more information on molecular mechanisms involved in a disease. A combination of their data, genomics and clinical outcomes indicates the impact of biomedical and health informatics on progress in stratified medicine. Nevertheless, storage conditions can affect results despite extraction of molecules can be easily obtained. Other techniques by which cancers maybe stratified are immunohistochemistry and polymerase chain reaction (PCR). They are routinely used in contrast to genomic, proteomic or metabolomic analysis. Immunohistochemistry utilizes antibodies that bind to a specific molecule. This is normally a cell-surface protein and appears with a unique colour under microscopic analysis. This technique can be performed using oestrogen receptor biomarker in breast cancer. Another example is PD-1 ligand in directing antibody therapy for patients with colorectal cancer and melanoma. Nonetheless, immunohistochemistry performed in clinical setting, diagnostic-grade antibodies are not used always. In relation to qPCR, they examine a desired DNA sequence in the sample that are normally cancer mutations. Similar to immunohistochemistry, they do not always perform using standardised processes. Thus, prospective techniques such as X-ray computed tomography, positron-emission tomography (PET) and magnetic resonance imaging do not require invasive procedures to obtain clinical samples. To observe the patient’s interior body, one examines what happens between electromagnetic radiations with the body. 18-fluorodeoxyglucose (FDG), a PET-active glucose analogue that resides in malignant tumour tissues with enhanced metabolic rate. In combination with PET, FDG is useful for diagnosis and examining therapeutic response in many types of cancer such as lymphomas. From a bedside perspective, molecular profiling appears to be a potential technique in identifying biomarkers in renal cell carcinoma aiding in decision-making for kidney cancer patients illustrated in Figure 5. Molecular profile is an analysis of protein and gene expression and leads to developing novel targeted therapeutic response. 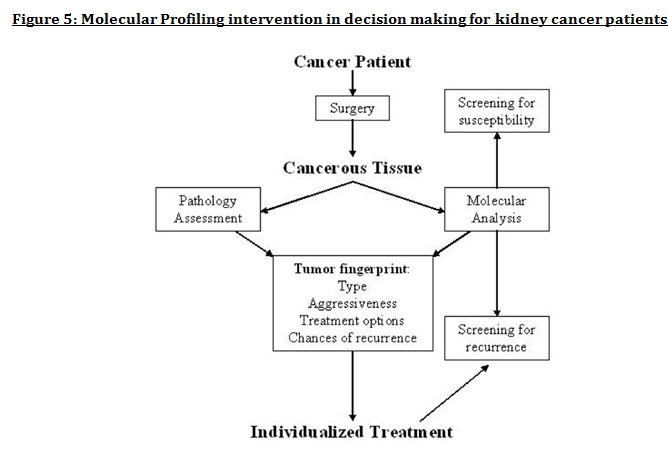 Furthermore, mutational stratification aids clinicians to determine which individuals will respond to which particular treatment. For instance, identifying KRAS in bowel cancer, Cetuximab and Panitumumab are observed to see if it implicated. Another example of how mutational stratification is likely to alter cancer treatment is gastrointestinal stromal tumour(GIST). Patients with GIST are prescribed with Imatinib. Some patients benefited where there was low GIST recurrence rates whereas others did not. Recent studies have demonstrated how mutational analysis is a predictive substance of recurrence-free survival. Patients with mutations in exon 11 of KIT gene, had more recurrence-free survival in comparison to patients with exon 9. Patients with wild-type GIST generally had disease but narrow sensitivity to Imatinib in most cases. Thus, risk-stratification and mutational analysis is necessary for optimising therapeutic approaches.
Lung cancer is another example of where mutational stratification has been used. It is the most common cause of mortality globally. According to statistics, 70% of NSCLC patients have durable effect and limited treatment obtained where 50% of them have an unknown cause. By using a specific genetic dependency screen one would be able to recognise vital somatic mutations. Findings discovered 3 kinases that have gain-in-function mutations in lung cancer mediating towards ERK pathway: PAK5, FGFR4 and MAP3K9. Consequently, mutated kinases prevent proliferation, inhibit downstream signalling events and eradicate lung cancer cells. Ultimately, stratified medicine plays a significant role in cancer treatment. Researchers are currently identifying more biomarkers to improve potential treatments. Cancer Research UK’s Stratified Medicine Programme entails molecular basis information of 9,000 tumours. It is co-working with pharmaceutical companies such as Pfizer to develop a national service model to routinely examine tumours for particular genetic variations. This will help clinicians with decision–making and aid researchers on how particular variations influence specific treatments. |
This project began as a facebook page sharing information about different illnesses, diagnosis and treatments. We are now doing short articles :)
Health stuffArchives
April 2020
Categories |
 RSS Feed
RSS Feed
