|
4/29/2015 Combined chemotherapy and immunotherapy shows promise for advanced prostate cancersRead NowChemotherapy can be very effective against small prostate tumors. Larger prostate tumors, however, accumulate cells that suppress the body's immune response, allowing the cancer to grow despite treatment. Researchers at the University of California, San Diego School of Medicine now find that blocking or removing these immune-suppressing cells allows a special type of chemotherapy -- and the immune cells it activates -- to destroy prostate tumors. This novel combination therapy, termed chemoimmunotherapy, achieved near complete remission in mouse models of advanced prostate cancer.
The study is published April 29 in Nature. Advanced or metastatic prostate cancer does not typically respond to chemotherapy. Prostate cancers also fail to respond to a promising new type of immunotherapy drugs, called checkpoint inhibitors, which disable cancer cells' cloaking mechanism so that a person's own immune system can better fight the tumor. This specific resistance is likely due in part to immunosuppressive B cells, which are more common in larger prostate tumors in mice, as well as in advanced and metastatic prostate cancer in humans. As the name suggests, these cells keep the immune system at bay, rendering most therapies ineffective and allowing malignant tumors to grow unchecked. In this study, researchers worked with three different mouse models of advanced prostate cancer. All three models were resistant to low doses of the chemotherapy drug oxaliplatin, which has the unique ability to activate cancer-killing immune cells. But when the researchers blocked the development or function of immunosuppressive B cells or removed them entirely before treating the mice with low-dose oxaliplatin, the prostate tumors were almost completely destroyed by the mice's own immune cells. The team got similar results when low-dose oxaliplatin was combined with a checkpoint inhibitor. "The presence of such B cells in human prostate cancer calls for clinical testing of this novel therapeutic approach," said Shabnam Shalapour, PhD, postdoctoral researcher and first author of the study. Prostate cancer is the second leading cause of cancer-related death in American men. About one in seven men will be diagnosed with prostate cancer during their lifetimes. "In addition to prostate cancer, similar immunosuppressive B cells can be detected in other human cancers," said senior author Michael Karin, PhD, Distinguished Professor of Pharmacology and Pathology at UC San Diego. "This indicates that B cell-mediated immunosuppression might be the reason several other cancers are also unresponsive to checkpoint inhibitors, raising the hope that chemoimmunotherapy will have broader applications for many cancer types." Reference: University of California, San Diego Health Sciences. "Combined chemotherapy and immunotherapy shows promise for advanced prostate cancers." ScienceDaily. ScienceDaily, 29 April 2015. <www.sciencedaily.com/releases/2015/04/150429132753.htm>.
0 Comments
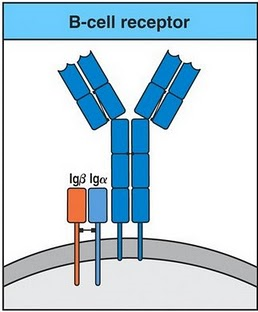 The adaptive immune response is split into 2 pathways: the humoral response & the cell mediated response. The cells related to these pathways also vary: in the humoral response involves B lymphocytes (B cells), while the cell mediated response involves T lymphocytes (T cells). B cells are derived from the bone marrow and circulate through the blood stream, spleen and lymph nodes. B cells produce antibodies and each antibody is specific to that B cell. Antibodies can be in two forms: excreted (IgG, IgA) or expressed on the cell surface of the B cell (IgM, IgD). B cells also have receptors on the surface, this receptor along with the antibody form signalling complexes. The receptor is made up of two proteins: Igα & Igβ- antigen binds to Ig – Igα & Igβ initiate intracellular signalling events to activate B cells. T cells are produced in the thymus however precursor T cells are produced in the bone marrow and migrate to the thymus located in the mediastinum, once matured T cells will travel around the body. There are two types of T cells that derive from the thymus which can be distinguishable based on the molecules present on the cell surface. Helper T cells express a molecule called CD4 on their cell surface, therefore known as CD4 T cells (T helper cells). The other type of T cells express a molecule called CD8 on their cell surface, therefore known as CD8 T cells (known as cytotoxic after activation). CD4 & CD8 T cells use a receptor called T cell Receptor (TcR) to recognise antigens. The TcR is different to the antibody and the genes that code for it are on different chromosomes. The TcR is made up of two glycoprotein chains called α & β. Both chains have a similar structure to Ig, as the TcR has a variable and constant domain. TcR is always present on the surface of the T cells. Different T cells will recognise different antigens as each TcR will have different variable regions. T cells recognise antigens that are associated with molecules on the surface of cells called ‘major histocompatibility complex’ (HMC). MHC refers to a region of the DNA and is located on the chromosome 6 in humans. All vertebrate species have an HMC, and a unique name is given to it. In humans the MHC is called HLA (human leucocyte antigen). MHCs are split into 3 classes: class I, II & III. The CD4 &CD8 bind to the non-polymorphic region of the MCH to get stronger bonding. Once infected the first response will be dealt with B cells (primary response). All B cells differ from each other depending on the Ig variable region of the antibody. The antibody of the cell will bind to the antigen of the pathogen or foreign particle. Once activated, the B cell will undergo clonal selection (create the specific antibody), it will proliferate and differentiate into plasma B cells (effector cells) and B memory cells. The effector cells are involved in the phagocytosis of the pathogen. The B memory cells stay in the body and activate during the secondary response, if the same pathogen was to infect again. Once the B cell has ingested the pathogen it will go through antigen processing and presentation. Endogenous antigens are produced within the cell (viral proteins) and are processed and presented by Class I MHC. Exogenous antigens derive from outside the cell and are processed and expressed by Class II MHC molecules. All nucleated cells express class I MHC. Proteins are fragmented in the cytosol by proteosomes. The fragments are then transported across the membrane of the endoplasmic reticulum by transporter proteins. Synthesis and assembly of class I heavy chain and beta2 microglobulin occurs in the endoplasmic reticulum and transported to the cell surface. A limited group of cells express class II MHC, which includes the antigen presenting cells (APC). The principal APC are macrophages, dendritic cells, and B cells. The exogenous proteins are taken in by endocytosis are fragmented by proteases in an endosome. The alpha and beta chains of MHC class II are synthesized and assembled in the endoplasmic reticulum. Then transported through the Golgi to reach an endosome where the peptide fragments from the exogenous protein are transported to the cell surface. Infected cells present foreign antigen to CD8 T cells. The MHC Class I (antigen) is recognised by TcR (CD8 T cell). This activates the CD8 T cell; it then proliferates and differentiates to cytotoxic T lymphocyte (CTL). The CTL produces cytoplasmic granules containing enzymes (granzymes) and perforin. The CTL releases perforin that makes holes in the plasma membrane of target cell, the granzymes enter the target cell (via perforin pores) and triggers aptosis of the target cell. CD 4 T cells specialise in antigen presenting cells (APC) present antigen to CD4 T cell. The MHC Class II (antigen) is recognised by TCR (CD4 cell) but this does not activate the CD4 T cell yet. Another signal is required which is the interaction of CD80/CD86 on APC with CD28 on T cells. Once activated the CD4 T cells synthesises and secretes cytokine (interleukin 2 (IL2)) and expresses receptors for IL2. The IL2 causes proliferation of activated CD4 T cells and differentiation of CD4 T cells into either Th 1 or Th2. Th1 help macrophages and B cells, Th2 help B cells. Th1 secrete IFNγ, this IFNγ activates macrophages that increase expression of MHCII and increase antigen presentation to CD4 T cells activating more CD4 T cells. The overall effect of this will be the amplification of the immune response. 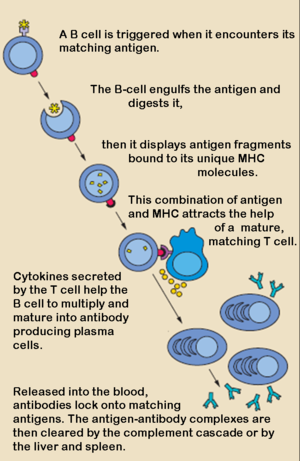 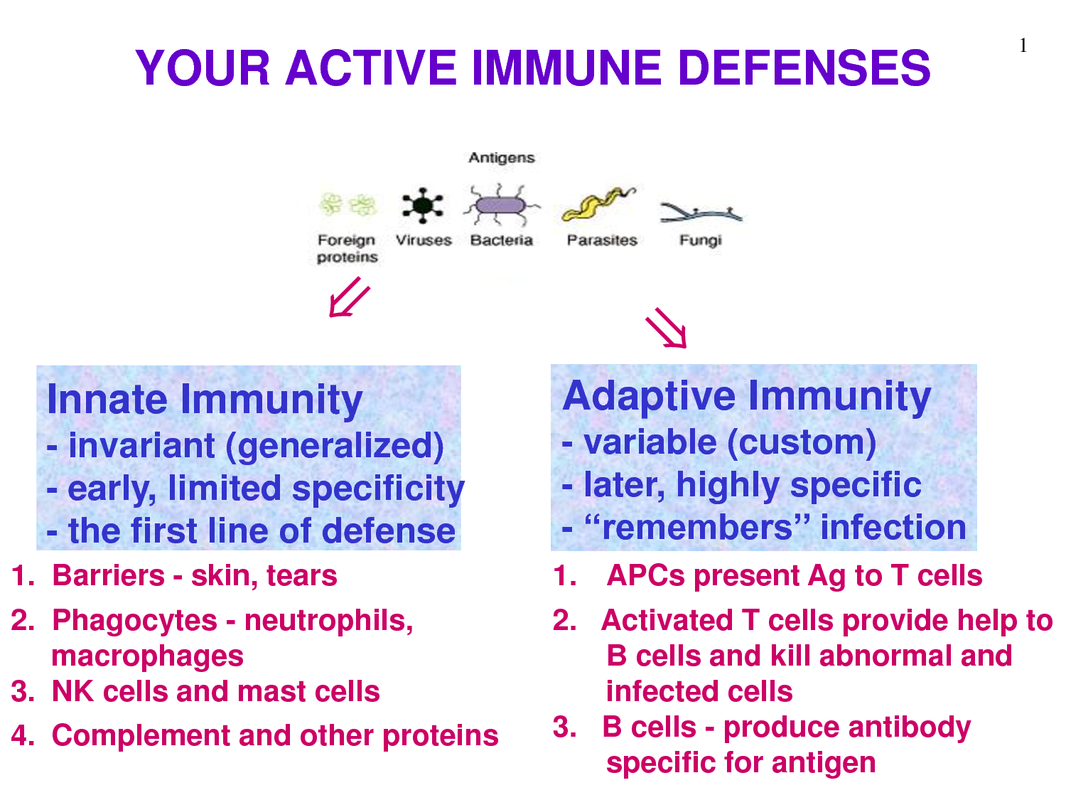 The immune system is the body’s way of fighting off invading pathogens. The immune system is composed of two parts: the innate immune response & the adaptive immune response. It is called the innate immune response as it is the pre-existing defence mechanisms that help prevent infection by pathogens or to create defence against an infectious agent. ‘Innate’ because it is present before an infection is occurs. The innate response in non-specific (whatever the pathogen: the response is always the same). It can be defined as the body’s first line of defence against pathogens. The physical, chemical & biochemical barriers are part of the innate response. It is divided into 5 stages: (1) Awareness of the infection (2) Immediate response to the infection (3) Delayed response (if immediate is not effective) (4) Elimination of pathogen (5) Provision of immunity Many cells and proteins in the body are part of the innate immune system. They provide two functions: 1) they are able to recognise the presence of invasion 2) provide immediate cellular response. One of the main types of cell involved is macrophages: these are created in the bone marrow and are found in most tissues. Another is neutrophils, which can also leave the blood stream and enter damaged or infected tissue. Mast cells and dendric cells are also involved. Cells related to the innate response have receptors that recognise pathogens based on their characteristics. One type of receptor is called ‘mannose receptor’, which is a C-type lectin carbohydrate binding protein that recognises complex carbohydrates. CD-14 is another type of receptor that acts as a Co-receptor with TLR4 (toll like receptor) in detecting bacterial liposaccharides. TLR are a family of receptors that recognise a variety of pathogens (TLR1 – bacterial lipopeptide, TLR2 – peptidoglycan, TLR3 – dsDNA). Recognition is only useful if it helps in the elimination of the pathogen or if it limits its replication. The response once recognition is achieved is phagocytosis. Phagocytosis is the ingestion and destruction of the microbe. Phagocytosis is done by macrophages & neutrophils. Phagocytosis is split into four steps: attachment of the phagocyte to the particle to be phagocytosed, ingestion : by extending the membranes around the particle and engulfing it taking it into a vacuole, then killing the phagocyte and degrading it by using the enzymes present in the vacuole. Instead of phagocytosis, another process that can occur is the secretion of proteins known as cytokines, which are produced in response to pathogen stimuli. Sometimes there are not enough macrophages present to eliminate the pathogen, so additional phagocytes are called that have a variety of proteins. This response is known as the inflammatory response. Leukocytes have a unique ability to move around the body, in & out of blood vessels & tissues. The control of where these cells go is very important and is achieved by adhesion molecules & chemotactic agents. Adhesion molecules bind to each other in a specific manner and enable cells to interact with each other. Adhesion molecules include: glycoproteins (lectins –super binding molecules that can be expressed on leukocyte or endothelial cells) & Integrins (hetrodimeric proteins consisting of alpha & Beta chains that are expressed on the leukocytes). Extravasation is the process of cells leaving the bloodstream, crossing the endothelium layer and entering the tissue. This is split into 3 stages: (1) Rolling neutrophils: normally travel in the centre of the blood stream away from the endothelium. Once inflammation occurs, it will cause vasodilation disturbing blood flow causing the neutrophils to bump along the endothelium (rolling motion). Inflammatory mediators such as TNF-α, the endothelial cells are activated to express P-selectins & E-selectins on their surface. These selectins bind to sialyl-Lewisx on the surface of the neutrophil slowing it down and making it roll along the endothelium. (2) Activation and Firm attachment: the binding of the sialyl-Lewisx is not strong enough for the neutrophil to adhere to the endothelium. To achieve a strong attachment, a LFA-1 integrin on the neutrophil binds to the ICAM-1 on the endothelium. Before the LFA-1 can bind, it has to go through a conformational change. To do this it must bind to IL-8 (interleukin). IL-8 is a chemokine and produced in response to an inflammation. Some of the IL-8 are in the extracellular matrix on the endothelial surface and can bind to IL-8 receptors present on the neutrophil surface. Once conformation has occurred, LFA-1 can firmly bind to ICAM-1 on the endothelium. (3) Transendothelial migration: Once the neutrophil is attached to the endothelium, it squeezes between the endothelial cells making contact with the basement membrane and releases enzymes that digest away the membrane allowing the leukocyte to enter into the tissue. Complement system is made up of a number of plasma proteins that play a role in resistance to infection. It consists of pro-enzymes and other factors that activate each other in order to produce a variety of active proteins. The proteins involved are called C1-C9. Different complement pathways exist: classical, lectin & alternative. All pathways start off differently but have a common end stage. The end product is to form a MAC (membrane Attack Complex). This is the generation of a pore in the membrane that will result in the lysis of the cell. The pores allow ions and small molecules through, but not proteins. There is an influx of water into the cell leading to the lysis ‘bursting’ of the cell. 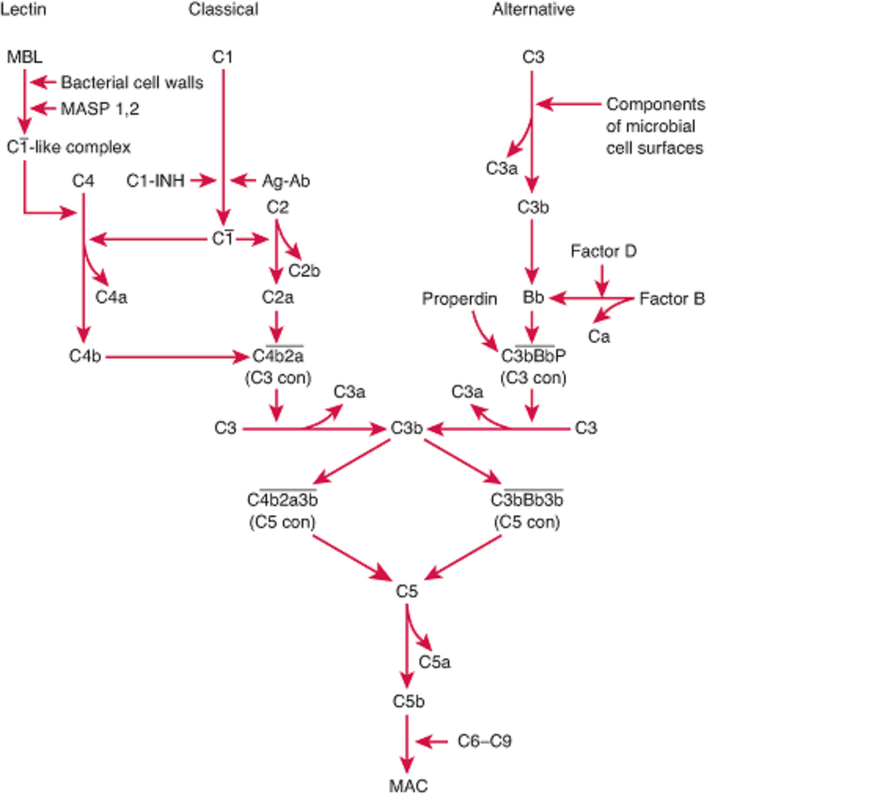 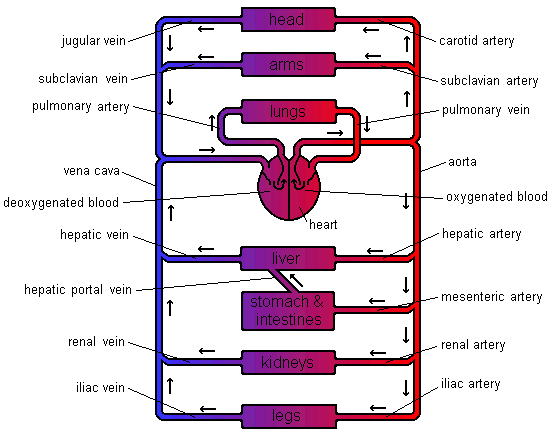 The function of the circulatory system is to transport materials around the body. There are many materials that need transporting. These include oxygen, carbon dioxide, nutrients (such as glucose and amino acids), hormones and waste chemicals such as urea. These substances are transported in blood through blood vessels. The blood is forced around these vessels by a pump - the heart. There are different types of blood vessels. Arteries - take blood away from the heart. Veins - take blood towards the heart. Capillaries - small vessels connecting arteries & veins. (1mm thick). Venules – smaller vessels of the veins. Arterioles – smaller vessels of the arteries. The blood travels around the circulatory system in a series of parallel circuits so that the blood travels from the heart, through an organ before returning to the heart. If the blood went through each organ in turn the organs near the end of the chain would not receive as many nutrients as the organs first in line. This is because the first organs would take out the nutrients leaving fewer for the organs that follow. There is one exception to this. The blood leaving the stomach & intestines first goes through the liver. The Liver receives its own blood supply, but this second supply gives the liver a chance to absorb any extra nutrients the body needs to store as well as neutralising any toxins that have been absorbed before they can wreak havoc throughout the body. Heart Structure The heart is really two pumps stuck together. There are two chambers to each side of the heart. The first chamber is called the atrium (atria - plural) and is the smaller of the two chambers. The larger one is called the ventricle. This chamber is the more powerful of the two as it forces blood out of the heart. The left-hand side receives deoxygenated blood from the body. The job of the left-hand side of the heart is to pump blood to the lungs to pick up oxygen and get rid of carbon dioxide. As the lungs are close by the pump does not need to be very strong. The right-hand side receives the newly oxygenated blood from the lungs and has to pump it around the rest of the body. As the distances are greater and in the case of the upper body, blood flow is against gravity, the right-hand side needs to be more powerful. 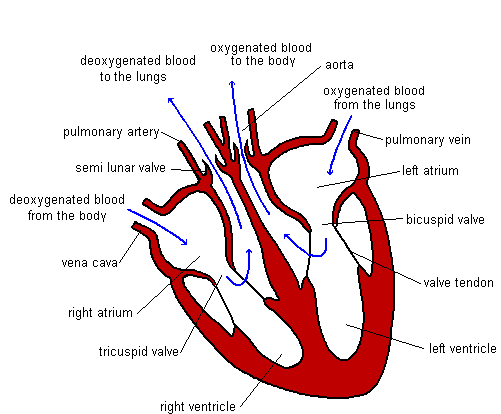 Heartbeat When the heart beats it takes in blood from the veins and forces it into the arteries. The heart is really two pumps stuck together. Each pump has two chambers. When the right atrium contracts, the same happens to the left-hand side. The same is true when the right ventricle contracts. The blood must flow through the heart in one direction. Blood enters the atria from the veins and is then forced into the ventricles. The ventricles force the blood into the arteries. There are a number of sphincter muscles and valves that prevent blood flowing the wrong way. The valves are a little like parachutes. When blood flows the wrong way the valves bulge out, blocking the path. Heartbeat involves three distinct stages: 1) relaxation phase - diastole 2) atria contract - atrial systole 3) ventricles contract - ventricular systole Events in Phase Diagram (only one side shown) DIASTOLE 1) The atria and the ventricles relax. 2) The semi-lunar valves close, preventing back flow into the ventricles. 3) The elastic walls of the aorta & pulmonary artery contract, forcing blood towards the body & the lungs. 4) Blood from the veins flows into the atria, which begin to fill. Deoxygenated blood enters the right atrium, and oxygenated blood flows into the left atrium. ATRIAL SYSTOLE 1) The atria contract, forcing blood into the ventricles, which fill. 2) Sphincter (ring) muscles closing off the vena cava and the pulmonary veins prevents backflow from the atria into the main veins. VENTRICULAR SYSTOLE 1) The ventricles contract, forcing blood into the aorta & pulmonary artery. 2) The main heart valves (tricuspid & bicuspid) are forced shut, so preventing backflow into the atria. This happens because the pressure of blood in the ventricles is higher than the pressure in the atria. The valve cords prevent the valve being pushed back too far. 3) The walls of the aorta & pulmonary artery expand. Blood Vessels Blood vessels are tubes, which carry the blood around the body. There are different types of blood vessels. Arteries carry blood away from the heart. These vessels split up into smaller ones called arterioles. Arterioles split up into tiny blood vessels called capillaries. It is from these vessels that movement of particles to & from the blood takes place. Capillaries join together to form larger vessels called venules which join together to form veins . 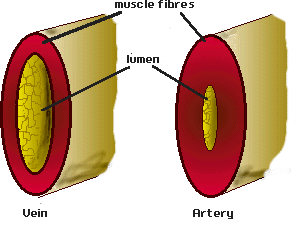 Heart Problems
There are a number of problems the heart can suffer from. Heart Murmur A leaky valve causes this. This means that some blood actually flows the wrong way. In minor cases this is not too much of a problem. If the leak is very bad it can cause major problems with blood flow around the body and may need corrective surgery. Pacemaker There is a special part of the heart found in the wall of the right atrium, which helps control, the speed and regularity of heartbeat. This region is called the Pacemaker as it helps control the speed of heartbeat. Sometimes problems can occur with this making the heart beat irregularly. An artificial pacemaker can be fitted to help correct this problem. An electrode is fitted to the atrium and another to the base of the ventricles. The artificial pacemaker sends out regular pulses of electricity down these electrodes to stimulate the heart to beat regularly. Heart Disease The heart is a muscle, which needs a good supply of food & oxygen in order to keep working. This is brought to the heart by the blood. If the supply of blood is halted or restricted in anyway the heart can quickly tire and then stop. This is a cardiac arrest (heart attack). A cardiac arrest can occur for a number of reasons. A high calorie diet results in excess fat in the body. Some of this fat ends up being deposited on the lining of the blood vessels. These fatty deposits can become calcified. This causes the vessels to become narrower. This problem is known as atherosclerosis. Having narrower blood vessels raises the blood pressure & the heart must work harder. If the blood vessels of the heart become blocked the blood flow to the heart will be reduced or stopped completely. Stress can increase the risk of heart failure. When under stress the heart has to beat faster. If this situation goes on then the heart is put under a great deal stress and this can lead to the heart stopping due to fatigue. Lack of exercise also increases the risk of heart disease. This is because the heart needs to be exercised like any other muscle. If it is not exercised the heart may not be able to cope when it needs to beat quickly (like running for a bus). Smoking increases the risk of heart disease because chemicals in smoke make it more likely for the blood to clot, even when still inside the body. This can cause blockages and so lead to heart failure. There is also a genetic factor. If there has been a history of heart disease in your family then this increases your chance of getting the disease. |
This project began as a facebook page sharing information about different illnesses, diagnosis and treatments. We are now doing short articles :)
Health stuffArchives
April 2020
Categories |
 RSS Feed
RSS Feed
