|
Atherosclerosis is the development of atheromatous plaques in the inner arterial wall. It is the underlying reason for the pathophysiology and aetiology of many arterial diseases particularly coronary artery disease (CAD) where these plaques partially or completely block arteries. This limits the oxygenated blood supply to myocardium causing over 90,000 UK deaths a year despite rates decreasing since 1970s (BHF,2009). There are two main coronary arteries (right and left) arising from aortic sinus; the anatomy of coronary artery is shown in Figure 1a. 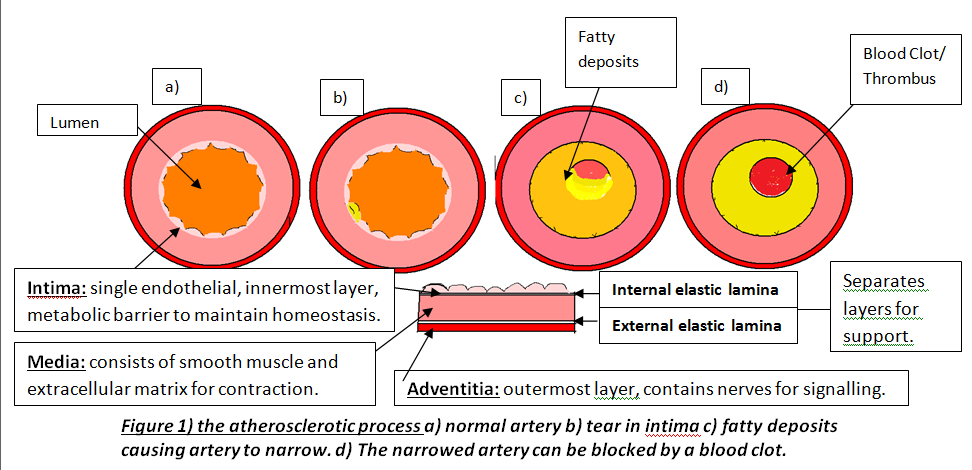
Atherosclerosis occurs in three major stages: fatty streak, plaque progression and disruption. Factors such as smoking cause endothelium to produce superoxide anions that interacts with other molecules. Superoxides are reactive oxygen species and free radicals of dioxygen due to unpaired electron (Widmaier,E. 2008:pp.84). This causes oxidative stress leading to endothelium dysfunction, allowing lipoproteins, calcium and fibrous tissues to enter and modify intima; Figure 1b. This initial damage increases CAD risk and initiates leukocyte recruitment primarily monocytes and T lymphocytes to enter inflammatory site. Monocytes differentiate into macrophages and secrete growth factors, platelet-derived growth factor (PDGF) and transforming growth factor-β (TGF- β), and have LDL-receptors to engulf lipids forming foam cells (Lilly,L. 2007 pp.126). These foam cells accumulate to form yellowish fatty streaks; Figure 1c. Plaque growth progresses when smooth muscle migrates to intima. PDGF allows smooth muscle to proliferate for collagen synthesis whereas TGF- β stimulate the process losing the arterial wall’s elasticity (Lilly,L. 2007:pp.127). A fibrous cap forms protecting atheroma, causing an ischaemic condition called angina. Over decades, dispute occurs between growth factors and IFN-γ factor; an interferon released by leukocytes inhibiting collagen synthesis. Disruption occurs when plaques rupture triggering a coagulation cascade where thrombus and fibrin deposit in arterial wall further reducing lumen and cause coronary occlusion; Figure 1d. This can lead to myocardial infarction (MI) where inadequate blood supply to part of the heart causes myocardial necrosis and can be fatal. Other causes of CAD are risk factors that promote atherogenesis. Controllable factors include diet, exercise and obesity. Obesity increases risk because abdominal fat enhances low-density lipoproteins (LDL) production and heart workload. Studies show that a third of CAD patients in developed countries are due to obesity emphasising its impact (BHF, 2008). As well as being an independent factor, it can trigger other factors, for instance, cholesterol where high LDL and triglyceride levels inside coronary arteries increase plaque formation. Low high-density lipoproteins (HDL) levels raises risk because epidemiological studies show that high HDL levels enhances endothelium function by preventing cholesterol entry (Brubaker,P. 2002:pp.9). There are also uncontrollable factors that contribute to CAD, for instance, gender and age. Women have higher HDL2 levels, a more cholesterol rich, than men preventing cholesterol entry and lowering CAD risk. Studies show 40% of deaths in 65-74 years old are due to CAD because myocardium cardiac function has decelerated, myocardium becomes less efficient and cardiac muscle (BJN, 2009). Individuals at risk of CAD are diagnosed using different examinations after experiencing symptoms such as chest discomfort where it spreads to arms and other areas; MI is identified when discomfort is beyond 15 minutes (Julian,D. 2005:pp.116). Clinical history and electrocardiogram (ECG) is needed because ECG records heart’s electrical activity by placing electrodes on arms, legs and chests detecting characteristic changes. For instance, ST segment lowers when there is myocardial ischaemia but elevates when MI initiates; Figure 2. 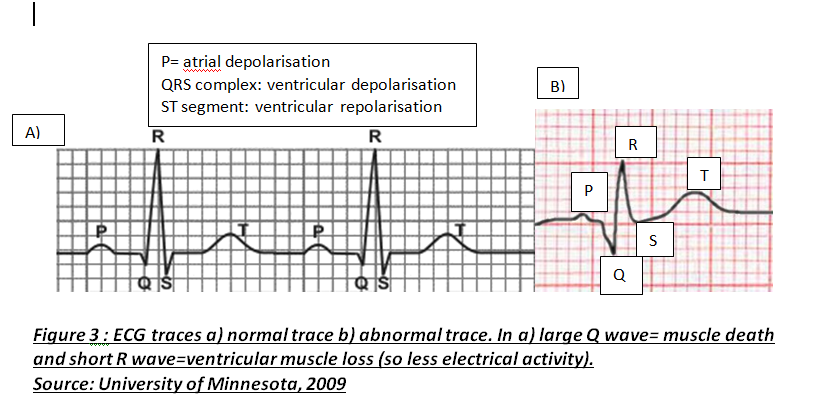
Another diagnosis is cardiac markers where high enzyme concentrations in cardiac tissues indicate myocardium necrosis. Tropinin T and I regulate cardiac muscle contraction and are mainly tested because they are sensitive and raise their serum activity when they detect any muscle injury (Julian,D. 2005:pp.112).
Treatment of CAD aims to improve coronary circulation by dilating coronary arteries which lowers pressure and myocardial oxygen demand and this reduces heart work. Drugs like nitrates have this pharmacological effect by relaxing smooth muscle whereas other drugs like atorvastatin lower LDL cholesterol by inhibiting HMG-CoA reductase; enzyme responsible for cholesterol synthesis (Kendall,M. 1998:pp.109). However, atorvastatin can cause myositis which affects muscles emphasising how medications can cause side-effects. If medications fail to work, surgery is needed. Coronary artery bypass grafting (CABG) involves using a vessel, normally saphenous vein, which bypass narrowed arteries providing an alternative route for blood flow. In 2002, mortality rate for Coronary Artery Bypass operations was 1.8% highlighting how surgery is effective (Barrett,D. 2006:pp.212). However, studies show that preventing modifiable factors by lifestyle adjustments are more effective than other treatments. Stopping smoking, maintaining healthy weight by exercising and eating low-saturated fat diet helps reduce cholesterol, blood pressure and controls glucose levels if diabetic. Ultimately, researchers are investigating possible new factors and cardioprotective drugs which emphasises the epidemic’s extent.
0 Comments
Leave a Reply. |
This project began as a facebook page sharing information about different illnesses, diagnosis and treatments. We are now doing short articles :)
Health stuffArchives
April 2020
Categories |
 RSS Feed
RSS Feed
