What is Obesity?Obesity is a condition where a person has an abnormal high triglyceride amount stored in adipocytes (fat cells) under the skin. Fulurija et al. reported it being one of the leading global health issues that result from a combination of genetic susceptibility, lack of exercise and high-energy food that are becoming increasingly available. Recent epidemiological studies suggest there is a causative relationship between obesity and the incidence of certain cancers including melanoma. However, the mechanism of melanoma is unknown despite obesity’s effect in progression of other cancers such as breast, colon and liver have been widely investigated (Pandey et al.) What is malignant melanoma? 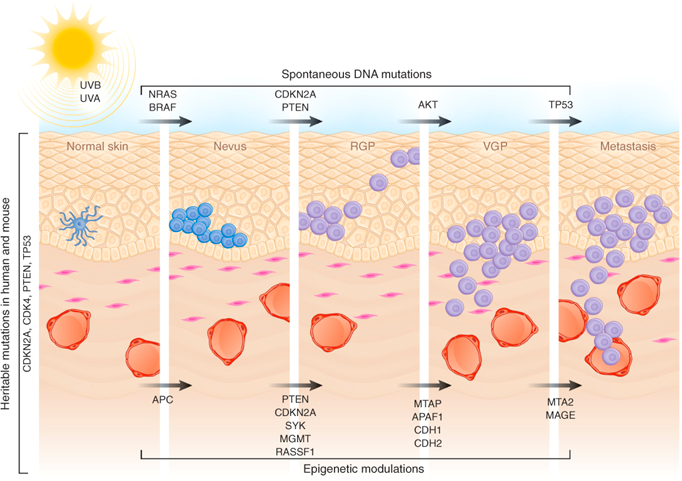
Malignant melanoma (MM) is a rare skin cancer that occurs in the following stages: Radial growth phase (RGP): Multiple clusters of abnormal melanocytes termed atypical moles cause a dysplastic naevus syndrome to arise which spreads horizontally within the epidermis across the basement membrane shown in Figure 1. If melanocytes are kept in epidermis, it is termed in situ melanoma (Oakley 2012). Vertical growth phase (VGP): With time, malignant melanocytes metastasize and proliferate through the basement membrane into the dermis and subcutaneous tissues. (Oakley 2012). Metastasis: as VGP develops, melanoma becomes thickened and raised; it metastasizes and colonizes to lymph nodes via the lymphatic system or other organ tissues such as the lungs, liver and brain via blood to develop a secondary cancer shown in Figure 2 (Khushiro 2012). This depends on the depth of cell that penetrated the skin (Oakley 2012). 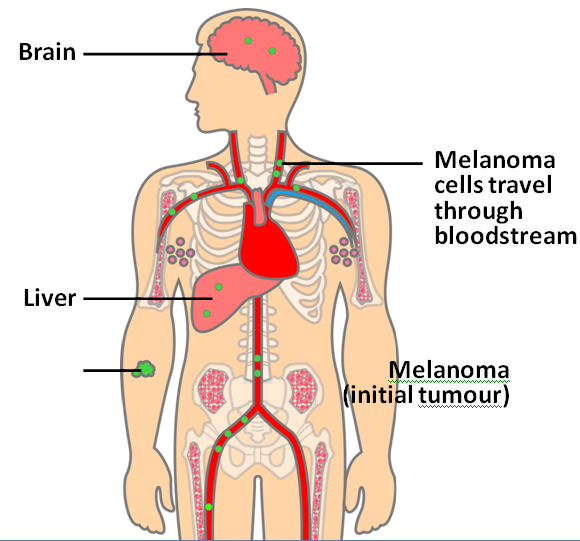
Figure 2: Malignant melanoma (Mee 2012)
Fact box: How is melanoma diagnosed?It begins with examining the mole using ABCDE (Asymmetry, Border, Bleeding, Colour, Diameter, Evolve) checklist to distinguish between a normal mole and melanoma. Normal moles are round, single-coloured whereas most melanomas have multi-coloured, irregular-shaped moles shown in Figure 3. They can be itchy or tender and bleed or crust. Further testing includes biopsies, microscope examination, X-ray, magnetic resonance imaging (MRI) and computerised tomography (CT) and blood tests (British Association of Dermatologists 2011). DNA microarray technology allows identifications of genes involved in tumourgenesis; mRNA that encodes for proteins such as TRP-1, melanoma antigen gp65, monoxcyte chemotactic protein 1 and melanoma differentiating antigen WAF1. With advances in microarray, gene expression regulation that takes place from a normal melanocyte to malignant melanoma can be studied accurately. This indicates how microarray can explain molecular mechanisms of tumour progression and genetic defects involved in MM and holds promises in melanoma care to improve screening methods and develop treatments using gene-directed therapy (Kim 2002). 
What are melanocytes and how are they normally regulated? Melanocytes are one of the predominant cell types located in the epidermis shown in Figure 4. They produce a pigment called melanin that functions to protect the skin and is responsible for the natural skin colours; this process is called melanogenesis (Cancer Research UK 2011). 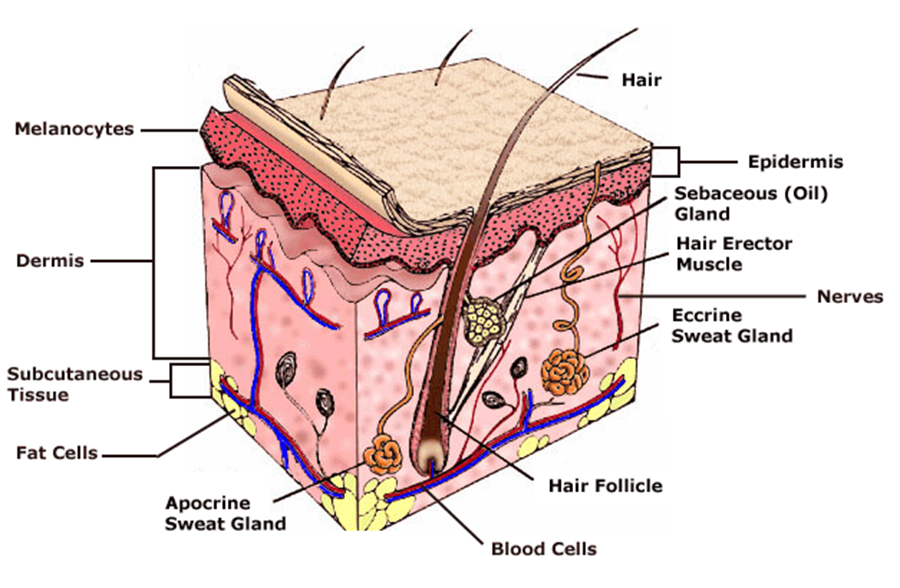
Figure 4: Skin Structure (American Skin Association 2012) The two main cell-signalling pathways that are important in the differentiation, survival and function of melanocytes are RAS mitogen-activated protein kinase (MAPK) pathway and phosphatidylinositol 3 kinase (AKT/PI3K) signalling pathway shown in Figure 5. 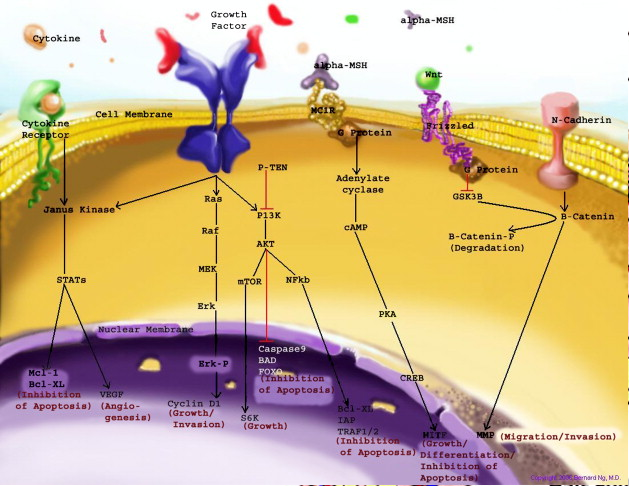
Figure 5: Regulatory processes involved in melanin synthesis (Carlson 2007) Growth factors bind to their specific receptors to activate RAS proteins which sequentially stimulate a phosphorylation cascade of cytosolic protein kinases. It begins with the downstream target called RAF then mitogen-activated protein kinase (MEK1/2) which then acts on extracellular-related kinases (ERK). ERK also interacts with (AKT/PI3K). Phosphorylated ERK kinases are translocated to the nucleus to regulate transcriptional activity of genes that promotes cell cycle progression and proliferation. The PI3K-AKT pathway mediates cell survival signalling via growth factors such as PDGF, NGF, and IGF-1 (Carlson 2007). Phosphatase and tensin homolog (PTEN) is a specific phosphatase that inhibits growth factor signalling by dephosphorylating the plasma membrane lipid phosphatidylinositol 3,4,5-trisphosphate (PIP3) in target proteins to produce phosphatidylinositol 4,5-bis phosphate (PIP2). PIP2 acts as a second messenger and phosphorylates serine/threonine protein kinases AKT. AKT can up-regulate mTOR (mammalian target of rapamycin) for cell growth and S6K, and NFκβ to inhibit apoptosis (Carlson 2007). α-MSH-MC1R (alpha-melanocyte stimulating hormone – melanocortotropin 1 receptor) pathway is also involved in melanocyte regulation. Melanocortins consist of α-MSH and adrenocorticotropic hormone (ACTH) peptides derived from a large precursor protein called pro-opiomelanocortin (POMC). Both MSH and ACTH can bind to MC2R which is coupled to G-protein alpha-s subunit which stimulates adenylyl cyclise (Convanse 2012). Adenylyl cyclase catalyses the cyclization of adenosine triphosphate (ATP) into the secondary messenger cyclic adenosine monophosphate (cAMP) shown in Figure 6. 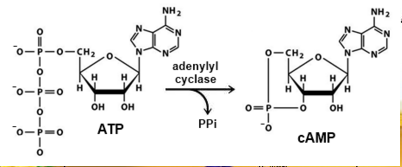
Figure 6: cAMP formation Fact Box: MSH and ACTH MSH is secreted by the intermediate lobe of the pituitary gland and stimulates melanin release and control melanin pigmentation. ACTH is a steroid hormone secreted by the anterior pituitary in response to corticortropin-releasing hormone from the hypothalamus and stimulates the adrenal cortext to secrete cortisol and has slight control over aldosterone; a steroid hormone from adrenal cortex (Bowen 1998). cAMP activates a cAMP-dependent enzyme called protein kinase A (PKA). PKA is a heterotetramer composed of catalytic and regulatory subunits shown in Figure 7. 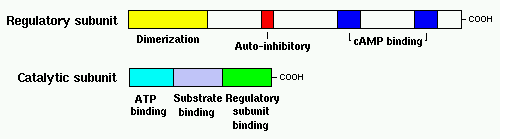
Figure 7: PKA structure PKA, in turn, phosphorylates and activates cAMP response element-binding protein 1 (CREB1). Phosphorylated CREB1 increases microphthalmia-associated transcription factor (MITF) expression in melanocytes, MITF transcription also regulated by Paired box 6 (PAX6) (Convanse 2011). MITF’s three-part structure aids in its function: Basic matif: attaches to specific DNA locations to help control melanocyte development, survival and function. Helix-loop-helix motif and leucine-zipper motif: important for protein interactions as MITF helps control activity of particular genes coding MRPs through interactions with M- and E-boxes located in the promoter regions of Tyrosinase-related protein 1 (TYRP1) and Melan-A (MLANA) (ref, ref). Within normal melanocytes, it also controls melanogenesis and cell cycle arrest whereas in melanoma it holds anti-apoptotic properties. Sp1 transcription factor (SP1) promotes Melanoma cell adhesion molecule (MCAM) expression in melanocytes. Consequently, all of these molecular mechanisms mediate melanocyte differentiation leading to melanin synthesis (Convance 2012) What is the link between obesity and malignant melanoma? The link between obesity and malignant melanoma is not fully understood and a number of studies were performed to investigate whether obesity increases MM incidence. Below are the current understandings of their relationship: Theory One: Leptin resistance Fact Box: What is leptin? It is a protein hormone with a mass of 16 kDa, encoded by the obese gene and is expressed predominantly by adipocytes. Tiny amounts of leptin are secreted in epithelials cells of the stomach and in placenta. It regulates body weight, metabolism and reproductive function. Leptin receptors are expressed in the hypothalamus, T lymphocytes and vascular endothelial cells to regulate body weight (Bowen 2006). Matriese et al. explained that leptin resistance is critical in obesity development and affects leptins’ functions. Most obese individuals have high plasma leptin concentrations that indicate leptin resistance. There are a number of defects that contribute to its resistance: · Defect in leptin transport across blood-brain barrier which reduces leptin’s availability to its receptor. · Defects in leptin receptor signal transduction such as impairment of STAT-3 phosphorylation · Reduced leptin receptor expression · Induction of leptin-signalling inhibitors such as SOCS3 (suppressor of cytokine signalling). Murpurgo et al. suggested that the increased risk of malignant melanoma in obese individuals is primarily due to leptin resistance which highlights the role of leptin in melanoma progression. Specifically, these individuals exhibit reduction of melanogenesis and the ability for melanocytes to repair DNA. Consequently, this increases MSH antagonists shown in Figure 8. All four antagonists lowers MSH activity and MCR 1 and 4, both receptors are members of the five-member G-protein coupled melanocortin receptor family and MCR1 is critical for melanogenesis and melanocyte DNA repair. 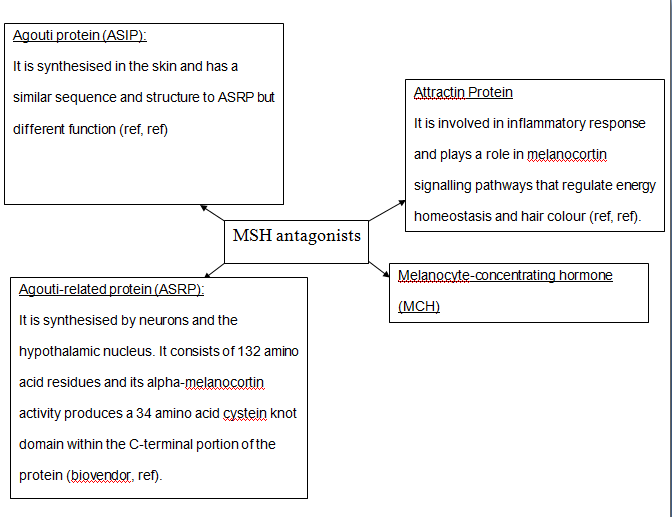
Figure 8: MSH antagonists Theory 2: Cav-1 and FASN involvement Pandey et al. found that diet-induced obesity enhances melanoma growth and was associated with increased Cav-1 and FASN expression. Both are co-ordinately regulated where Cav-1 interacts with FASN in melanoma cells to control proliferation. This demonstrates how diet-induced obesity effects melanoma progression and also indicates how obesity affects critical pathways in melanoma. Cav-1 (caveolin-1) is one of the three integral proteins of the caveolin family. They form hetero- and homooligomers that interact with cholesterol and other lipids to form the sphingolipid-enriched plasma membrane structure. They are involved in cholesterol homeostasis, cell adhesion, apoptosis and interact with a number of signalling molecules for example Gα subunit, tyrosine kinase receptors, PKCs, Src family tyrosine kinases, and eNOS (cell signal). Fatty acid synthase (FASN) catalyses long chains of fatty acids synthesis from acetyl-CoA and malonyl-CoA. It produces lipids in the liver for metabolically-active tissues or storage in adipocytes (cell signal). Theory Three: Melanoma risk is associated with serum leptin levels However, Gogas et al. findings opposes Matriese et al. because they revealed that elevated serum leptin levels in obese individuals was linked to melanoma risk and not with obesity. This result may be due to BMI and adipose tissue may not be one and the same. The major factor that influences serum leptin concentration is adipose tissue mass. Leptin synthesis is affected by several factors: insulin, tumour necrosis factor alpha, glucocorticoids, gonadal hormones, catecholamines and prostaglandins. They also found that: · Leptin expression can be stimulated under hypoxic conditions and often occur in solid tumours. · Leptin connects obesity with melanoma development by stimulating proliferation; it enhances endothelial cell migration and angiogenesis. Leptin stimulates angiogenesis independently and in interaction with two growth factors: vascular endothelial growth factor (VEGF) and fibroblast growth factor-2 (FGF-2). In normal angiogenesis, during embryogenesis vasculature development consists of new endothelial cells associated into tubes by the process termed vasculogenesis in addition to sprouting (angiogenesis) of new vessels from existin vessels. Subsequently, normal vasculature becomes quiescent. Similar to normal tissues, tumours need nutrients, oxygen and the ability to excrete metabolic wastes and carbon dioxide. The tumour-associated neovasculature created by angiogenesis address these needs. · Leptin increases endothelial cell growth and suppress apoptosis through a bcl-2 dependent mechanism shown in Figure 9 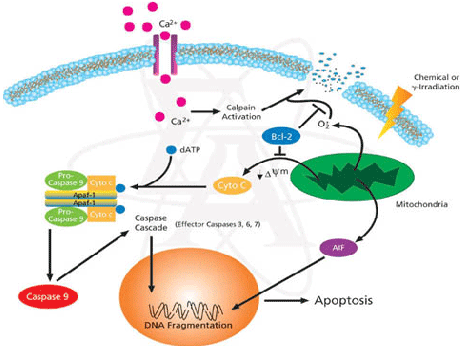
Figure 9: Bcl-2 plays a role in the intrinsic pathway which involves mitochondrial protein release such as cytochrome C interacting with other cytosolic protein factors: apoptoic protease activating factor-1 (Apaf-1) and procaspase-9 to stimulate the association of a caspase-activating complex called a apoptosome. This induces activation of caspase-9 and initiates the apoptotic caspase cascade. By interacting with Bax, Bcl-2 can inhibit pro-apoptotic activity by inhibiting Bcl-2. · Leptin can act as a mitogen (an agent that induces mitosis) or a migration-inducing factor in different cell types such as smooth muscles, normalized and neoplastic colon cells and normal and malignant mammary epithelial cells. Furthermore, Gogas et al. findings needed to be confirmed in future studies to enable the understanding of pathophysiological mechanism and the role of the above factors in predicting melanoma risk. Fact box: What are VEGFs? They are dimeric glycoproteins with a mass of 40kDa and have five forms: VEGFA, VEGFB, VEGFC, VEGFD and PLGF (Mee 2012). Its roles are shown in Figure 10 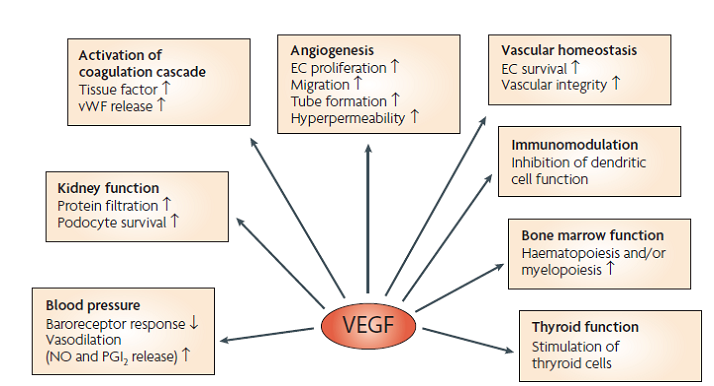
Figure 10: VEGF functions Fact box: What are FGFs? FGFs activates its receptors (FGFRs) on endothelial cells and can induce angiogenic factors from other cell types to indirectly stimulate angiogenesis. Low FGF levels are necessary to maintain vascular integrity. Abnormal FGF signalling enhances tumour angiogenesis and mediates escape of tumour vascularisation from VEGF (Mee 2012). Theory Four: Obesity promotes melanoma progression with or without leptin’s presence Brandon et al. (2009) found limitations in previous studies as their experiments were performed in vitro with high leptin concentrations. They concluded from their mouse studies that the relationship between obesity and melanoma growth was unclear and leptins’ role in promoting melanoma progression is still uncertain. This was due to their following findings: · Obesity promoted melanoma progression whether leptin was present or not. · Energy restriction prevents obesity to reduce tumour size · Leptin deficiency in obesity attenuates progression which correlates with Matriese et al. findings. · Leptin receptors were expressed in melanoma cells but leptin could not be detected as little was produced. However, there is a possibility that leptin interacts with VEGF as their expression was increased in obese mice which suggests obesity increases melanoma growth rate by mechanisms that involve regulating VEGF pathway. However this mechanism does not occur in all cancers. · The leptin found in tumours were derived from host leptin that was removed in the tissues from immune cells that infiltrate the tumour or circulation. Theory Five: Obesity creates a pro-cancerous microenvironment Previous studies suggested that obesity promotes melanoma development by creating a pro-cancerous microenvironment consisting of high levels of growth and inflammatory factors: cancer-associated fibroblasts (FACs), macrophages (TAMs), and adipocytes (Kushiro 2012). Adipocytes secrete inflammatory cytokines that recruit macrophages to initiate angiogenesis by secreting matrix metalloproteinases (MMPs) collectively known as matrixins are calcium-dependent proteases which are synthesizes as a inactive proenzymes and are activated by cleavage of a pro-petide. It hydrolyses extracellular matrix (ECM) and basement membranes of neighbouring blood vessels (Kushiro 2012). MMPs 2 and 9 specifically degrades collagen type IV component of basement membrane. This enables metastasising tumour cells to move through ECM (Mee 2012). A discovery! Recently, miR-126, a member of small non-coding RNA (microRNAs) was revealed to inhibit endothelial recruitment by suppressing a set of cancer genes that activate endothelial MMP is controlled by an increased expression on a transcriptional level. Thus, microRNAs expressed by cancer cells could shape the tumour and metastatic microenvironment (Mee 2012) Theory 6: Obesity increases metastasis by promoting a mesenchymal cell phenotype The Epithelial-to-Mesenchymal Transition (EMT) normally functions in the formation of the body plan and differentiation of multiple tissues and organs and contribute to tissue repair (Mee 2012). It consists of an epithelial-type cell that obtains a mesenchymal phenotype which gives it migratory and invasive ability needed for cancer progression and higher metastatic ability (Khushiro 2012). The mesenchymal phenotype is associated to cells’ ability to migrate to distant organs allowing differentiation into multiple cell types during metastasis initiation and development. EMT in cancer progression is characterized by activation of transcriptional factors such as TGF-β1, Snai1, Twist and Slug abnormally. They aid in inhibiting cell-to-cell adhesion that maintains cell attachment to each other by reducing E-cadherin, an anchorage protein that increases expression of mesenchymal markers such as Vimentin shown in Figure 11and increase invasiveness of tumour cells (Kushiro 2012). Khushiro 2012 found obesity may increase the metastatic ability of melanoma by promoting a mesenchymal cell phenotype. This finding was revealed after finding: · high levels of resistin, insulin, tPAI1, IL-6, TNF-α, and MCP-1 in obese serum which increases invasive ability of melanomas. · They also found that ob/ob serum increased the expression of Snai1 and Twist. Both Snai1 and Twist are strongly associated with EMT and metastasis of melanomas. It increased MMP9 activity and decreased the expression of E-cadherin and the metastasis suppressor gene Kiss1. 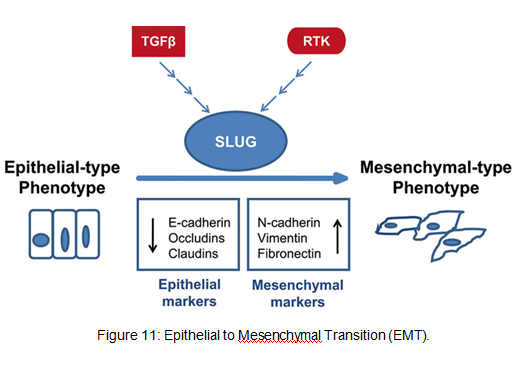
Treatment for obesity and obesity-linked cancers? Over 120 different types of anti-obesity drugs have been tested in clinical trials but only Orlistat has been proved to be safe and effective. It blocks the action of a protein used to digest fat. The undigested fat is passed out with stools to avoid gaining weight but it will not necessarily cause one to lose weight. However, currently approved anti-obesity drugs show only limited efficacy, generally facilitating no more than a 5–10% reduction of body weight and are often associated with side-effects. A new therapeutic target called Gastric inhibitory peptide (GIP) may hold promising novel therapy for long-lasting obesity treatment and also show that vaccination against GIP is safe and effective after recent studies have shown that GIP receptor-deficient mice are finally protected from diet-induced obesity. Normally, GIP promotes triglyceride clearance from the circulation which is partially mediated by its ability to stimulate lipoprotein lipase activity. However prospective pre-clinical safety studies is necessary before the therapy can be introduced in humans (ref, ref) In relation to anti-cancer therapy, researchers from the University of Manchester (2008) recommended national cancer plans that entail the following to reduce obesity, decrease cancer incidence and increase survival: · Restriction for high-calorie and low-nutrient food advertisements · Limited access to unhealthy foods · Promote physical activity in schools and workplaces. · Avoiding alcohol as it contains high calories which increase weight. New Discovery! A yellow compound called Curcumin mediates anticancer and obesity activities but are not yet been publicized. It modulates multiple molecular targets and reverses insulin resistance as well as other symptoms that are associated with obesity-related cancers. Curcumin mediates multiple molecular pathways, and is considered to be of therapeutic value in the treatment and prevention of obesity-related cancers. Conclusion Overall, to summarise what studies have shown about the link between obesity and malignant melanoma:
· Obesity increases metastatic ability of melanoma by enhancing Cav-1 and FASN expression. · It creates a pro-cancerous microenvironment of growth and inflammatory factors to initiate angiogenesis. · Leptin resistance and its high levels in serum in obese individuals. · However, Brandon et al. argues the previous finding and found that obesity promoted melanoma progression whether leptin was present or not. Thus, current molecular mechanisms of how obesity associates with melanoma development and progression is unclear and ongoing research is necessary to understand melanoma pathogenesis in order to establish effective therapeutics with less side effects. Obesity may have a causative relationship with malignant melanoma but it is not the main risk factor. Gogas et al. reported that MM incidence in Caucasian individuals is increasing globally making it the most increasing cancer in white populations except for lung cancer among women. Dark-skinned people have a lower risk because their melanocytes have more melanin thus more natural protection, despite having the same amount of melanocytes as Caucasian people. Other factors include the ‘sensitive’ skin phototype (fair skin, easily to burn and unable to tan), dysplastic nevi presence, family history, previous melanoma and immunosuppression (Cancer Research UK 2011).
0 Comments
Leave a Reply. |
This project began as a facebook page sharing information about different illnesses, diagnosis and treatments. We are now doing short articles :)
Health stuffArchives
April 2020
Categories |
 RSS Feed
RSS Feed
